
Pregnancy and family planning
In the modern era pregnancy and family planning is a complex consideration. There is a great amount of helpful evidence to assist with women and couples making informed choices and your GP is available to discuss all of them.
Choosing your contraception
There are various methods of contraception available in Australia including:
Long acting reversible contraception (LARC)
Contraceptive implant
· A contraceptive implant is a LARC. It is a small plastic rod that is placed under the skin of your upper arm. It slowly releases a low dose of the hormone progestogen, which stops your ovaries releasing an egg each month. You will notice a change to your period or it may stop altogether.
· The implant will last for three years and is an excellent method of preventing pregnancy. It can easily be removed and won’t stop you from getting pregnant later on.
Intra uterine device (IUD)
· An IUD is a small contraceptive device that is placed in your uterus. An IUD is also a LARC. There are two kinds of IUD:
o copper IUD (Cu-IUD) – lasts for 5 to 10 years
o hormone-releasing IUD – lasts for 5 years.
· An IUD stops sperm from reaching and fertilising an egg.
· It also changes the lining of your uterus so a fertilised egg won’t stick to it.
· An IUD can be easily removed by a doctor or nurse and won’t stop you from getting pregnant later on.
· The copper IUD may make your periods heavier and the progestogen IUD will make your periods lighter or stop them completely.
Oral contraceptive pills
There are two main types of contraceptive pills that must be swallowed every day.
The combined oral contraceptive pill (COC)
· The COC has two hormones (oestrogen and progestogen) that stop the ovaries releasing an egg each month and thickens the mucus in your cervix. The COC may also reduce acne and menstrual bleeding and pain. The combined pill is very good at preventing pregnancy when used correctly.
The progestogen-only pill (mini pill or POP)
· This pill has only one hormone and works by changing the mucus at the entrance to the uterus so that sperm cannot pass through to fertilise the egg.
· The POP is different to the COC because it doesn’t stop you ovulating (releasing an egg). The POP is very good at preventing pregnancy when used correctly.
Emergency contraceptive pill (sometimes called the ‘morning-after pill’)
· If you had sex without contraception, or you had trouble using your regular method (missed pills or broken condom), you can take an emergency pill to prevent pregnancy.
· Emergency contraceptive pills are best taken as soon as possible after unprotected sex, ideally within 24 hours (1 day), but still work well within 96 hours (4 days). You can take ECP within 96 to 120 hours (5 days) after having unprotected sex, but it won’t be very effective. The emergency pill is available from the chemist with no prescription.
Vaginal ring
· The vaginal ring is a soft plastic ring that is inserted into the vagina. It slowly releases low doses of two hormones, oestrogen and progestogen that are absorbed into your body. It works in a similar way to the COC to prevent pregnancy. The vaginal ring is inserted for three weeks. You remove it for one week to have your regular period. After the week without the ring, you insert a new one.
Contraceptive injection
· Depot medroxyprogesterone acetate (DMPA) is a long-acting progesterone hormone that is given as an injection every 12 weeks.
Barrier methods
Male condom
· The male condom is a fine rubber or synthetic sheath that is worn on an erect penis. It collects the sperm and stops them entering your vagina and uterus. You can buy condoms from a chemist or supermarket. Condoms reduce the risk of both pregnancy and STIs. Condoms are effective if they are used correctly. If they are not used correctly, which is common, you have a significant risk of getting pregnant or catching an STI.
Female condom
· A latex-free female condom is also available. It fits loosely in your vagina and stops sperm from entering your uterus. A soft removable ring helps to insert it as well as keeping it in place. A large flexible ring stays on the outside of the vagina covering the vulva (outside of the vagina). If used correctly, the female condom reduces the risk of both pregnancy and STI. It is more expensive and less readily available than the male condom.
Diaphragm
· A diaphragm is a shallow, cup-shape made of silicone. In Australia there is one size diaphragm available sold as Caya®. It is used with a special gel (jelly-like material, sold as Caya Gel®)..
Sterilisation
· Both men and women can have a simple operation to make them sterile. The operations are permanent. You would only have these operations if you don’t want any more children. For women, the operation involves blocking the fallopian tubes to stop the egg traveling from your ovaries to your uterus. There is also a procedure where tiny inserts are placed inside your fallopian tubes. This procedure can be done through the vagina and can be done while you are awake.
Before you fall pregnant
Take a look at this important information:
Getting pregnant and infertility
Fertility starts to decline for women from about the age of 30, dropping down more steeply from the age of 35. After 35 years, the proportion of women who experience infertility, miscarriage or a problem with their baby increases.
By the age of 40 only two in five of those who wish to have a baby will be able to do so. The average age at which women have in vitro fertilisation (IVF) treatment is rising. This reflects the increase in infertility due to age. However, the success rates of IVF treatment for women over 40 using their own eggs are low, and have not increased much over the past decade.
From a purely biological perspective, it's best to try to start a family before you're 35 years old. Men can remain fertile for much longer than women. Even though male fertility also declines with age, it tends to happen gradually for men. There is another important point to consider if you're trying for a baby when you're over 35. You have a higher chance of having a multiple pregnancy. In fact, the older you are, the more likely you are to conceive non-identical twins.
You may be delighted at the prospect of conceiving twins. For some women having a multiple pregnancy brings them their dream family in one pregnancy. But it is also worth bearing in mind that caring for twins is more demanding of your time, emotions and finances than caring for one baby. You may also need extra care during a multiple pregnancy.
Over 80 per cent of couples will conceive within a year if they stop using contraception and have regular sex. Regular sex means making love every two to three days throughout your cycle. This gives you the best chance of conceiving. About half of the women who don't get pregnant in the first year conceive during the following year, giving a pregnancy rate of 92 per cent within two years.
Figures for women aged 30 to 34 and aged 35 to 39 are fairly similar, with 94 per cent and 90 per cent conceiving within two years, respectively. Because natural conception rates are so good given time, it's usually recommended that you only seek help from your GP if you haven't conceived after a year of having regular sex (two to three times a week).
But if you are over 35, and finding that positive pregnancy test elusive, it is important to seek help from you GP sooner rather than later.
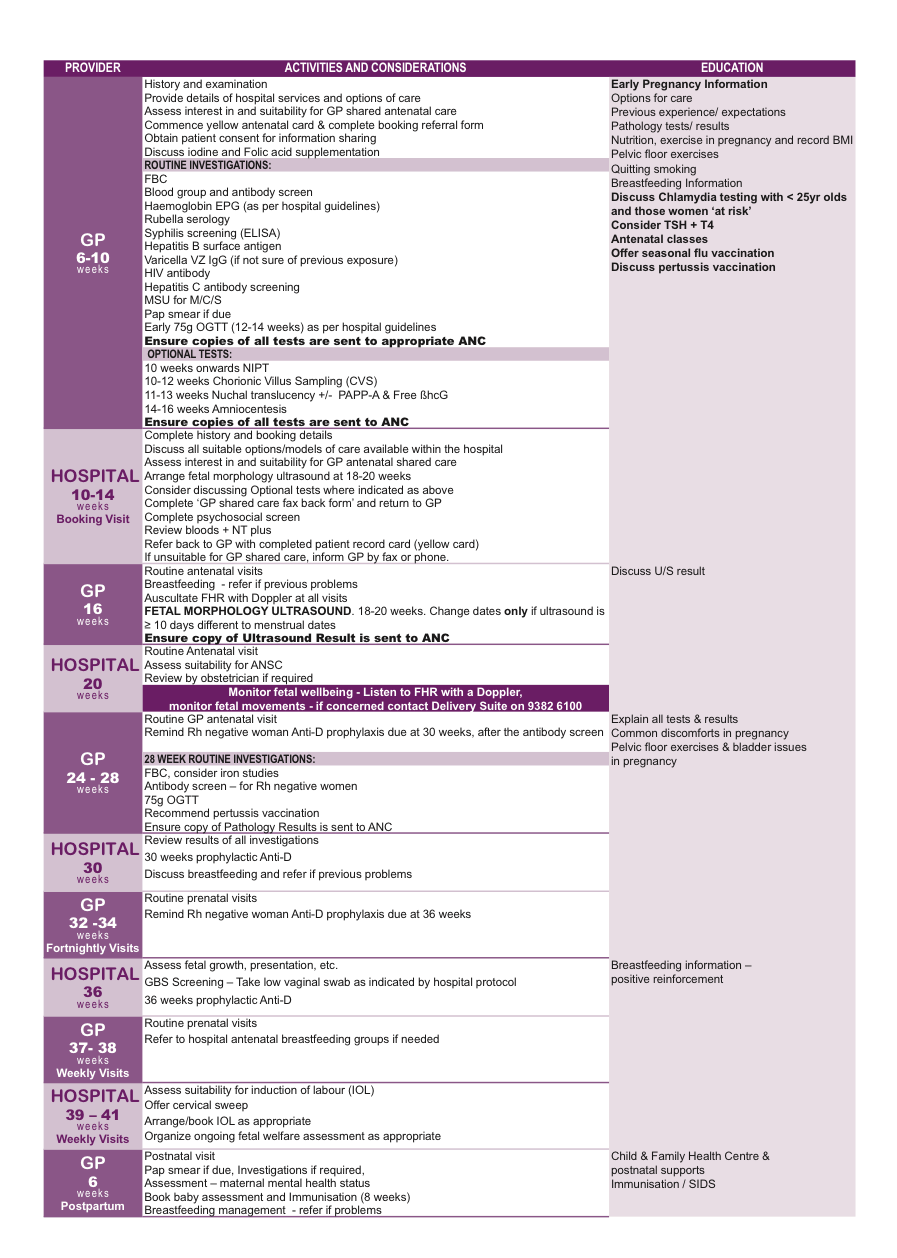
Pregnancy and shared care with your GP
Once you’re pregnant it’s important to enjoy the excitement, but also to attend your GP who will outline the medical agenda for the next 40 weeks to ensure you have the healthiest possible pregnancy for both you and your baby. A snapshot of the shared care program that your GP will facilitate between you and your nominated hospital is below. As you can see there is much to do, but your GP will take all of the anxiety away and carefully direct you along your pregnancy journey only focussing in on specific concerns should they arise.
Beyond the medical requirements that you will undertake throughout your pregnancy there are lifestyle and dietary considerations that your GP will guide you through.
After you have you delivered
This is where the fun and fatigue really begins! Postpartum care is very important and your GP is always there to help you with any concerns about your own body or the baby throughout this very important time. This is a joyous time, but it’s also a period of adjustment and healing for mothers.
Adjusting to motherhood
Adjusting to everyday life after the birth of a baby has its challenges, especially if you’re a new mother. Although it’s important to care for your baby, you also have to take care of yourself. Since a baby has to be fed and changed often, you may experience sleepless nights - It can be frustrating and tiresome. The good news is that you'll eventually find a routine. In the meantime, here’s what you can do for an easier transition:
1. Get plenty of rest. Get as much sleep as possible to cope with tiredness and fatigue. Your baby may wake up every two to three hours for feeding. To make sure you’re getting enough rest, sleep when your baby sleeps.
2. Seek help. Don’t hesitate to accept help from your partner, family, friends and of course you doctor during the postpartum period.
3. Eat healthy meals. Maintain a healthy diet to promote healing. You should also increase your fluid intake, especially if you are breast-feeding.
4. Exercise. Your doctor will let you know when it's OK to exercise. The activity should not be strenuous. Try taking a walk near your house. The change of scenery is refreshing and can increase your energy level.
Baby blues vs. postpartum depression
It’s normal to have the baby blues during the postpartum period. This typically happens a few days after giving birth and can last for up to two weeks. In most cases, you won’t be experiencing symptoms all the time, and your symptoms will vary. About 70 to 80 percent of new mothers experience mood swings or negative feelings after giving birth. Baby blues are caused by hormonal changes and symptoms may include:
· unexplained crying
· irritability
· insomnia
· sadness
· mood changes
· restlessness
When should you see a doctor?
The baby blues are different from postpartum depression. Postpartum depression occurs when symptoms last for more than two weeks. Additional symptoms may include feelings of guilt and worthlessness, and loss of interest in daily activities. Some women with postpartum depression withdraw from their family, have no interest in their baby, and have thoughts of hurting their baby. Postpartum depression requires medical treatment. Speak with your doctor if you have depression that lasts longer than two weeks after giving birth, or if you have thoughts of harming your baby. Postpartum depression can develop at any time after giving birth, even up to a year after delivery.
Coping with body changes
Along with emotional changes, you’ll experience body changes after giving birth, such as weight gain. Weight loss doesn't happen overnight, so be patient. Once your doctor says it's OK to exercise, begin with moderate activity a few minutes a day and gradually increase the length and intensity of your workouts. Go for a walk, swim, or join an aerobics class. Losing weight also involves eating healthy, balanced meals that include fruits, vegetables, and whole grains. Every new mother loses weight at a different pace, so don't compare your weight loss efforts to others. Breast-feeding can help you return to your pre-pregnancy weight faster because it increases your daily calorie burn. Talk to your doctor if you have questions or concerns about changes to your body during the postpartum period.
Breast engorgement
Your breasts will fill with milk a couple of days after birth. This is a normal process, but the swelling (engorgement) can be uncomfortable. Engorgement improves with time – but you may require advice from your midwives and lactation consultants after you deliver or your GP.
Constipation
Eat high-fiber foods to stimulate bowel activity, and drink plenty of water. Ask your doctor about safe medications. Fiber can also relieve haemorrhoids, as well as over-the-counter creams or sitting in a sitz bath. Drinking water helps ease problems with urinating after birth. If you experience incontinence, Kegel exercises can strengthen your pelvic muscles.
Pelvic floor changes
The area between your rectum and vagina is known as the perineum. It stretches and often tears during birth. Sometimes a doctor will cut this area to help your labour. You can help this area recover after your delivery by doing Kegel exercises, icing the area with cold packs wrapped in towels, and sitting on a pillow.
Sweating
Hormonal changes can cause night-time sweating after having a baby. Remove blankets from your bed to stay cool.
Uterine pain
A shrinking uterus after giving birth can cause cramping. The pain subsides in time. Ask your GP about safe pain medications.
Vaginal discharge
Vaginal discharge is typical for at least two to four weeks after giving birth. This is how your body eliminates blood and tissue from your uterus. Wear sanitary pads until the discharge stops. Do not use tampons or douche until your four to six-week postpartum appointment, or until your doctor approves it. Using these products in the immediate postpartum period may increase your risk of uterine infection. If you have any concerns they will be addressed by your obstetrics team or you GP.
Our doctors love helping bring happy and healthy babies into the world and caring for their parents.